The BRIC NS Student Seminar Series is an opportunity for students across Nova Scotia to share their completed or in-progress research.
Presentation Title: “Health Outcomes and Healthcare Access Experiences of Incarcerated and Recently Released Women in Rural Areas: A scoping review.” Presenter: Clare Heggie, MA, PhD Candidate
Clare Heggie is a PhD Candidate in the Department of Interdisciplinary Studies at the University of New Brunswick, supervised by Dr. Martha Paynter. Her research is focused on the health impacts of incarceration and criminalization on women and gender diverse people, and she has been involved in a number of projects examining the experience of accessing reproductive healthcare in prisons. She is a recipient of a Vanier Canada Graduate Scholarship from SSHRC. Date and time: October 16, 2025, 12-1pm, AST, via Zoom Webinar Registration – Zoom
Dr. Beth McDougall, PhD, will present: “Validation and Application of a Needs-Based Complexity Case-Mix System for Community-Based Primary Health Care Planning and Research » Beth McDougall is a Senior Epidemiologist with Nova Scotia Health Performance and Analytics and has worked in health research for almost 20 years. She recently completed her PhD in Epidemiology and Applied Health Research at Dalhousie University under the supervision of Dr. George Kephart and is set to graduate in October 2025. She is passionate about health, with research interests spanning primary health care, mental health and addictions, health services research and clinical trials. She particularly enjoys contributing to projects that advance evidence-based decision-making in healthcare. In her spare time, Beth loves hiking and keeping up with her energetic 16-month-old and playful Labrador Retriever.
[This essay was written by the Young Leaders Committee in Patient-Oriented Research (POR), a community of early career researchers and student-researchers supporting the scientific community and its members, whose mission is to promote the next generation of POR leaders by supporting POR capacity building, networking and mentorship, scientific production, and POR knowledge translation, as well as collaboration among its members.]
The “covidification” of research
The COVID-19 pandemic has shone the collective spotlight on health research. The media report daily on scientific advances supporting the fight against COVID-19: epidemiological data, clinical trials of treatments, vaccine development, etc. Many members of the scientific community in Quebec, Canada, and internationally have mobilized to address the emerging issues of this COVID-19 crisis, to such an extent that we are witnessing a rapid “covidification” of research: major investments in research on COVID-19 (e.g. pharmaceutical, basic science, specialized medicine), the creation of networks and platforms for sharing research on COVID-19, the suspension of several non-COVID-19 research activities, the cancellation or postponement of funding competitions for non-COVID-19 studies, and the reorientation of many research teams towards COVID-19.
This “covidification” of research reflects an intention to answer pressing questions in the fight against COVID-19, but it also poses certain risks. Of course, research on epidemiology, vaccines, and treatments for COVID-19 is essential. However, it is also crucial to address issues of health service organization, quality of care, health equity, and the social aspects of this crisis. We need to avoid an “over-covidification” of research; let’s not forget that the non-COVID issues still affect patients and many challenges in our health systems have been amplified by this health crisis. Moreover, neglected or postponed health care and the delays in management of patients’ health problems will bring new challenges.
The importance of patient-oriented research
In this context, patient-oriented research (POR) is once again critically important. The upheavals we are experiencing underscore the need to produce knowledge that addresses people’s concerns. POR can produce evidence on health care services and policies oriented towards improving the health and well-being of populations and health professionals. Yet POR, which involves a strong collaborative process, is on shaky ground. During the pandemic, we need to make sure patients, health professionals, and decision-makers can continue to participate safely, and significantly, in order to ensure the production of meaningful and relevant evidence. In our post-COVID society, it will be more important than ever to maintain strong links with patient-partners so that work currently on hold can resume and adapt to the emerging challenges facing patients and the health system.
What is POR?
Patient-oriented research (POR) mobilizes patients and multidisciplinary partners, focuses on priorities established by patients, and improves patient outcomes. POR aims to apply knowledge to improve health systems and health care.
Issues for the next generation of researchers
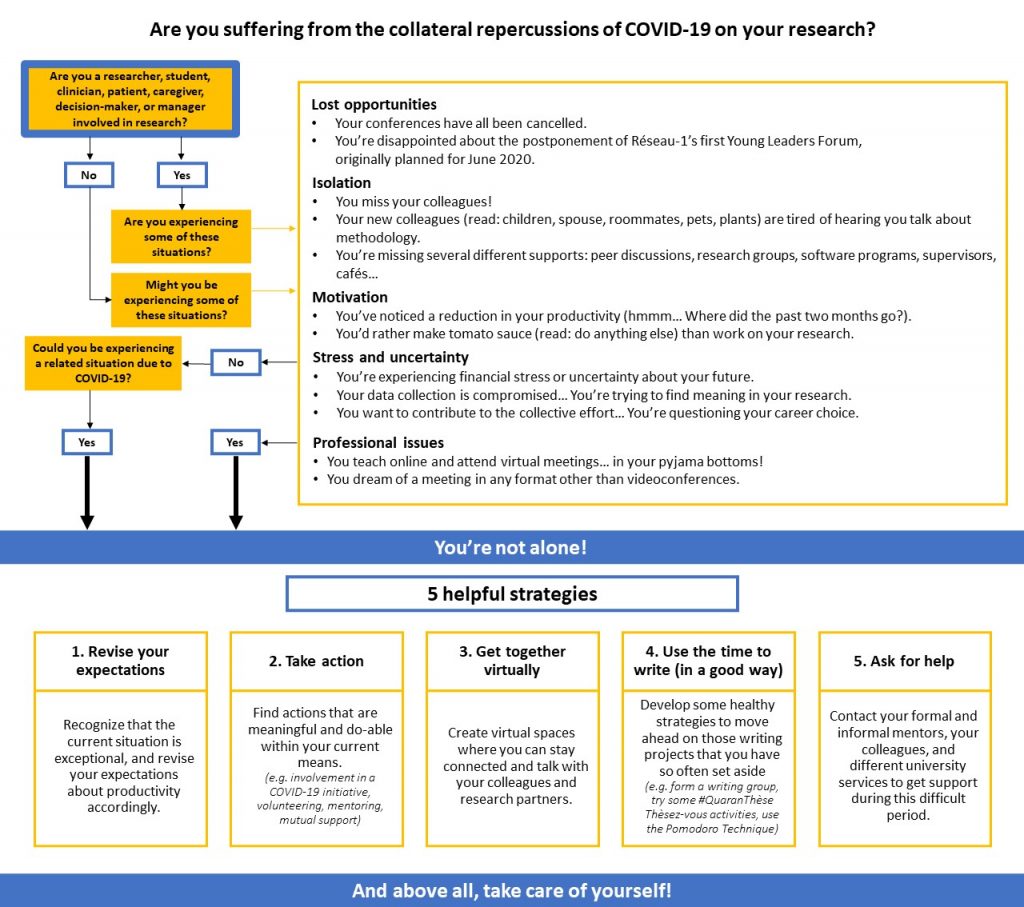
As early career researchers and student-researchers, this “covidification” of research has hit us head-on, and we are dealing with inevitable collateral effects (see our algorithm below). A loss of motivation and uncertainty about this situation have strained our capacity to be resilient and to adapt. Here are some examples of what we are experiencing: reduced job prospects and job insecurity in research; uncertain thesis defenses in formats that don’t do justice to the scope of the work and don’t allow for celebration commensurate with the effort; unreliable research funding due to the cancellation of various competitions; difficulties reconciling pro-COVID-19 research with our own research programs in a coherent manner; excessive project delays caused by the interruption of data collection; reduced ability to maintain links with patient-partners and other collaborators; the cancellation of networking events that are so valuable for our career advancement; a heavy workload generated by the move to online coursework; work–family balance issues related to working from home and the closure of schools and daycare centres; etc.
The next generation of researchers does not necessarily have the same resources and networks as experienced researchers to cope with these challenges. This situation contributes to a certain precariousness and can make research students and young researchers vulnerable.
Supporting the next generation of researchers
These upheavals contribute to weakening the next generation of researchers. Without additional support, there is a risk our generation of young researchers will crumble. Research supervisors, more experienced researchers, universities, research networks, and funding agencies all have a role to play in supporting the next generation of researchers, particularly in the current context.
It is crucial that student-researchers and early career researchers are afforded the support, flexibility, and understanding they need. Resources must be made available to us to carry out our work and plan our early career paths: more frequent follow-ups; formal and informal mentoring; support in reorienting our projects and data collection; setting priorities with regards to our objectives; flexibility in deadlines for grant and scholarship applications; consideration of work–family balance in scientific production; extension of grants and funding; etc. The creation of virtual spaces to facilitate collaboration, mutual aid, and networking can also strengthen a sense of belonging and reduce isolation. Innovative ways must be found to enable the next generation of researchers to attend training sessions, gain experience, demonstrate leadership, and engage in research. For example, the next generation can become involved in COVID-19 grant applications and projects if they are given opportunities by more experienced researchers or if their participation is encouraged by research networks and funding agencies. Granting agencies and universities could also be encouraged to show flexibility and support in maintaining and creating strategies to support the next generation of researchers in the short, medium, and long terms (e.g. competitions, funding, sponsorships, virtual events, mentoring, productivity support, career planning support).
An opportunity to rethink the research of tomorrow
As young POR researchers, we often experience discomfort and frustration with more traditional research structures and approaches that seem old-fashioned and partially out of step with the needs and realities of patients and health systems. We dream of research that is more agile, innovative, and interdisciplinary, conducted in collaboration with all holders of knowledge and experience (patients, clinicians, communities, managers, decision-makers, and researchers); research that is applied in real time to solve emerging problems, and where our performance as researchers is measured by the impact of our contributions and not just by the number of lines in our CVs. In short, “Research 3.0”, as Réseau-1 would describe it.
Amongst ourselves, we sometimes question our career choice: will research enable us to make a significant contribution to improving the health system and the well-being of populations? If the major research upheavals of recent months have proven one thing to us, it is that research can change, adapt to emerging needs, and be agile. This gives us renewed hope in research and its mission. Let’s take advantage of this crisis to rethink research, to innovate, and to make lasting changes that will maintain this agility and renewed relevance of research. We, the next generation of patient-oriented researchers, are ready to take on this challenge. Let’s not forget: we are not alone. We are part of a strong research community that is more important now than ever!
Mélanie Ann Smithman, Doctoral candidate, Université de Sherbrooke; Co-director, Capacity strengthening, Réseau-1 Québec; Fellow, Québec SPOR Support Unit
Isabelle Dufour, Nurse, Doctoral candidate, Université de Sherbrooke; Fellow, Québec SPOR Support Unit
Virginie Blanchette, Podiatrist, PhD; early-career professor, Université du Québec à Trois-Rivières; POR trainee
Jean-Christophe Bélisle-Pipon, PhD, Visiting researcher, The Petrie-Flom Center for Health Law Policy, Biotechnology, and Bioethics, Harvard Law School; Fellow, Health Law Institute, Dalhousie University; Invited researcher, School of Public Health, Université de Montréal; Fellow, Québec SPOR Support Unit
Samuel Turcotte, Occupational therapist; Doctoral candidate in clinical and biomedical sciences (rehabilitation option), Université Laval; Fellow, CIHR SPOR (transition to leadership stream) and Québec SPOR Support Unit
Mohamed Ali Ag Ahmed, MD-MPH, PhD; Postdoctoral fellow with the Research Chair on Chronic Diseases in Primary Care, Université de Sherbrooke
Ruth Ndjaboue,Postdoctoral trainee, Université Laval; Fellow, Diabetes Action Canada – a national patient-oriented research network
It’s still too early to measure all the impacts of the unprecedented crisis we are experiencing. But one thing is certain, if we accept the reports coming from the front lines: clinical practice will no longer be the same. The transition to telemedicine, which took literally two weeks, will finally bring us, by all accounts, into the 21st century and make it possible to deploy connected health care and a variety of telediagnostic platforms. We are finally entering the modern era. We are also beginning to see the collateral damage of remote practice: missed diagnoses, segments of the population falling below the radar. Here I offer a few thoughts on what I know best—family medicine—but I believe they are applicable to primary care clinical practice in general.
Telemedicine and connected health, for what objectives and what types of decisions?
Clinicians paid on a contract or salary basis have long known that many small problems could, in fact, be solved remotely. It’s a bit ironic that people are only discovering this now. I used to end every consultation day with a half-hour of returning calls to manage minor problems for patients I knew well. But I would have gotten into a lot of trouble, even with patients I knew well, without all the information that an in-person visit provides—gait, gestures, facial expressions, moments of silence—from the greeting in the waiting room to the good-bye with the hand on the doorknob, and the “By the way, doctor, for a while now I’ve been having this chest pain when walking.” To explain the craze for telemedicine—which by the way is mostly audio (over the phone) rather than “tele-” (video)—we hear all sorts of things, such as this poorly understood quote that “80% of diagnoses are based on history,” invoked to assert that the phone is sufficient in the majority of cases. This is a mistaken understanding of the clinical process, so well described by Epstein 40 years ago. While it’s still true that 80% of the clinical process is based on history, most often it takes a physical examination and sometimes a few laboratory tests to capture the missing 20% in order to arrive at the right diagnosis. Of course, connected objects and tools derived from artificial intelligence will make us even more efficient at a distance. But the intellectual task required for the clinical process is excessively demanding and complex. It calls for acquiring several types of information and “processing” them—in the computing sense of the term—and then linking this information with scientific knowledge obtained from research to decide on the most probable diagnosis or prognosis and the treatment most likely to be effective. This involves not only identifying symptoms but also understanding the person and their context. Symptoms are more of a narrative than a precise set of data.
Telemedicine, connected objects, and diagnostic applications derived from artificial intelligence (AI) will be particularly useful for facilitating the monitoring of known problems, reducing diagnostic and therapeutic uncertainty, and bringing certain medical advances to more remote areas. But these advances will not relegate the medical visit to the back burner anytime soon. In fact, according to Eric Topol in his essay “Deep Medicine,” the main benefit of these advances should be to make healthcare more humane than ever by freeing up healthcare professionals to focus on what is essential to the practice of “good medicine”: listening, understanding the whole person, and being compassionate.
Reducing inequalities: access to primary care services as a factor in equity
COVID-19 also exposed the weak links in our health care system. One of these was the inability to lessen the impact of health inequalities. More than ever, COVID revealed and deepened inequalities. Inequalities in disease severity accentuated by the dangerous mix of co-morbidity, poverty, and precarious living conditions. Inequalities in access to non-COVID related care and the resurgence of diseases responsive to prevention and early treatment. Access to primary care services is a protective factor against health inequalities. Unfortunately, in Canada and in Quebec, there is strong evidence that less advantaged people have more difficulty accessing a family physician and that lower socio-economic status, older age, ethnic origin, and being female are more frequently associated with poorer quality preventive and curative services. As it is, many clienteles are unable to breach the fortresses that medical offices and health care institutions have sadly become. While the use of telemedicine will certainly help reduce certain geographic inequalities in access, there is a danger that this mode of practice will deepen inequalities by reducing access, already difficult, for the homeless, persons with mental health and addiction problems, the elderly, the less educated, and recent immigrants. It will take creative thinking to reach out to these people where they live, on the street, in their homes, and to find ways to make our practice environments welcoming to them. COVID-19 has already shown how courageous and inventive front-line practitioners can be. Some striking examples of this are projects supported by Réseau-1 (https://reseau1quebec.ca/projets/projets-sur-la-covid-19/) and the Foundation for the Advancement of Family Medicine (https://fafm.cfpc.ca/fr/programme-sci-covid-phaseone/).
Learning by doing: The importance of research in primary care
Paradoxically, the technological advances promoted by COVID-19 could have a deleterious impact if not used wisely, both clinically and in terms of problems they could create of unequal access to front-line services. So we need to learn from these practice transformations, in order to identify those that really add value and those that cause us to backslide. When I completed my master’s degree in epidemiology, my research director, Ms. Jacqueline Fabia, a great epidemiologist, gave me this advice, the importance of which I was slow to realize: “Keep good records. Important discoveries come from careful observation of practice. Your records are a mine of information.” Careful observation is also about measuring the impact of COVID and our new clinical and organizational practices from the patients’ perspective.
No, clinical practice should not continue as it was, and there must be no going back once the pandemic is over. But to truly move forward and take advantage of this unprecedented crisis, we need to return to the art of clinical practice and the value of research rooted in practice. This is the only way to learn “while building the plane.” Back to the Future.
Marie-Dominique Beaulieu, C.Q., M.D.,CMFC, M.Sc., FCMF, Professor Emeritus, Department of Family Medicine and Emergency Medicine, Université de Montréal